

A Critical Gap in Infection Prevention:
The Overlooked Hazard of Infant Mattress Contamination
Whitepaper as appearing in the Leap Frog December Newsletter
Presented by: Deva Rea MPH, BSN, RN, CIC
Healthcare associated infections (HAIs) are unfortunate events that are oftentimes preventable. Infection prevention practices typically involve multifactorial interventions to reduce HAI risk. Neonates and infants, especially those born prematurely, are at an increased risk of infection due to their immature immune systems and underdeveloped physical defenses including skin barriers. Invasive medical devices or procedures further increase their infection risk. HAIs in neonates remain a major challenge in the Neonatal Intensive Care Unit (NICU). Across multicenter surveillance studies, up to 18% of NICU admissions experience at least one HAI. Bloodstream infections are the most common and clinically significant type of infection in this population. ¹,² The majority of infections are classified as late-onset sepsis. Late-onset sepsis develops 72 hours after birth and is predominately attributed to pathogens in the infant’s environmental surroundings.³
The financial and clinical burden of neonatal sepsis is substantial. According to the Agency for Healthcare Research and Quality (AHRQ), the average total hospital cost for neonatal sepsis inpatient stays increased from $36,700 in 2016 to $56,300 in 2021, with average lengths of stay rising from 11.8 days to 16.2 days. The annual in-hospital mortality was 225 infants nationally. Costs escalate further among very low birthweight infants and socially vulnerable populations. Each preventable infection avoided through environmental control reduces length of stay, downstream complications, mortality, and institutional costs.
Despite advances in hand hygiene, device management, and antimicrobial stewardship, there is a persistent under recognized environmental reservoir, the mattress. Environmental surfaces play an established role in pathogen transmission, and porous mattresses consistently demonstrate microbial contamination due to compromised integrity and cleaning failures. ⁴,⁵
The Regulatory Divide
In 2013, the U.S. Food and Drug Administration (FDA) issued a safety communication documenting more than 700 mattress-cover failures and multiple contamination-related events. The FDA emphasized that soft, porous mattresses may retain blood and body fluids and remain contaminated despite cleaning, noting that internal contamination is not visible on inspection.⁶ Although the communication focused on adult beds, neonatal and pediatric mattresses share the same construction vulnerabilities.
The Centers for Disease Control and Prevention (CDC) has stated that mattresses have a potential to become contaminated with body substances during patient care if the cover’s integrity becomes compromised. Mattress covers are typically made of a thin (1/50th of an inch), polyurethane material that can be compromised by wear and tear, disinfectants, and other factors. The goal of the cover is to protect the mattress core from becoming contaminated with body fluids and substances. The CDC emphasizes that a linen sheet is not considered a mattress cover, nor a barrier. Additionally, the CDC A Critical Gap in Infection Prevention: The Overlooked Hazard of Infant Mattress Contamination notes that patches for tears and holes in mattress covers are also not acceptable and do not provide an impermeable surface over the mattress. Another important detail is that sewn mattress cover seams do not provide an impermeable surface, which further emphasizes the need to inspect the foam underneath the cover. The CDC also recommends replacing mattress covers when they are torn or visibly stained, noting mattresses can be substantial environmental sources of infection and colonization.⁷
Despite these recommendations and guidance, there are still no infant or neonatal specific guidelines detailing how to prevent mattress contamination or how often incubator mattresses should be replaced. The CDC and The Joint Commission mandate adherence to environmental cleaning and reprocessing guidance found in the manufacturer instructions for use (MIFUs), but do not specify how to verify the effectiveness of cleaning these porous surfaces. Specifically, the CDC recommends using disinfectant products that are compatible with mattress-cover materials to ensure that the covers remain impermeable and undamaged.⁷ However, most often, harsh disinfectants are used, which rapidly erode the mattress cover, leaving it vulnerable to fluid penetration (Figure 1). Moreover, the standard method used to ensure mattress integrity is visual inspection. However, visual inspection’s value is limited and subjective. Many times, a mattress cover appears to be visually intact, but when the mattress cover is removed, substantial contamination is present (Figure 2). Unfortunately, true inspection cannot be fully achieved with most infant mattresses due to sewn or sealed seams. Infant mattresses that are sealed do not have the ability to be opened, which is a potentially major health hazard because they cannot be thoroughly inspected according to the manufacturer’s recommendations (Figure 3). Most infant mattresses also have an expected lifespan, but tracking is often ineffectual and many remain in service well past their intended use. This lack of clear guidance leads to contamination, infections, and neonatal vulnerability, underscoring a significant gap in infection prevention.
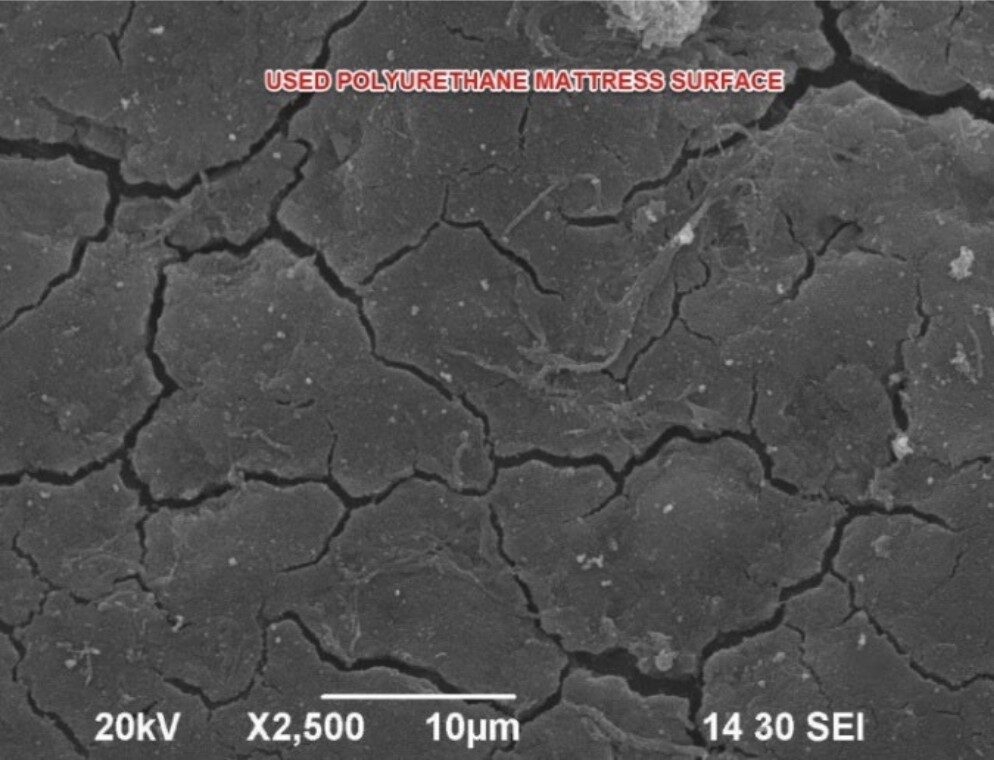
Figure 1: Example of surface damage due to disinfectant use

Figure 2: Fluid penetration into foam at mattress seam

Figure 3: Example of sewn mattress seam
Mattress Contamination in Healthcare: An Essential Focus
Mattress contamination with clinically significant pathogens in healthcare settings is well-documented and poses a significant risk for healthcare-associated infections (HAIs) and outbreaks, especially when cleaning and decontamination practices are suboptimal. Mattresses and bed surfaces can harbor pathogens such as methicillin-resistant Staphylococcus aureus (MRSA), vancomycin-resistant
Enterococci (VRE), Acinetobacter spp., Klebsiella pneumoniae, Pseudomonas aeruginosa, and Enterobacter cloacae, even after routine cleaning.⁸-¹¹ Environmental contamination, including mattresses, increases the risk of patient colonization and infection. Outbreak investigations have also been directly linked to mattress contamination, with epidemiologic evidence showing transmission of identical strains between mattresses and patients.⁹,¹⁰ A cluster of Clostridioides difficile infections from postpartum patients specifically implicated mattresses as the likely reservoir.¹² Mattresses are often overlooked compared to other non-porous surfaces such as bedrails, as critical reservoirs and as direct links to outbreaks when not adequately decontaminated.⁸
The most vulnerable infant and neonatal populations are also greatly at risk for infection due to persistent mattress contamination. Multiple studies have shown that mattresses and incubator surfaces in these settings can harbor pathogenic bacteria and fungi, even after routine cleaning and disinfection, leading to transmission of HAIs and outbreaks. As previously described, most infant mattress covers are sewn or sealed, which does not allow proper internal mattress inspection. Furthermore, evidence continually points to mattresses as being the most contaminated part of incubators.⁴,⁵,¹³-¹⁹ Sealed and sewn seams likely allow a perfect environment for biofilm development and persistent colonization. ¹⁹ Infant mattress covers with cracks, or even visibly intact, allow fluids and bacteria to penetrate within the mattress foam; serving as potential sources of infection.²⁰ This once again demonstrates that internal contamination is not detectable through visual inspection and cannot be reliably removed by routine disinfection.
One well described outbreak of an extended-spectrum beta-lactamase-producing Klebsiella pneumoniae (ESBL-KP) was identified in a neonatal care center that directly linked incubator mattresses to strains found in patients, even after cleaning. Outbreak control required mattress replacement and improved disinfection protocols, highlighting mattresses as critical reservoirs for pathogens and outbreak spread.⁴ Other robust studies directly demonstrate infection risk and outbreaks associated with mattress and incubator contamination in NICU and neonatal settings (Table 1).
Table 1: Summary of Select Mattress Contamination Studies in the Neonatal and NICU settings.
| STUDY | SUMMARY |
|---|---|
| Cadot et al. (2019) | During a 3-month ESBL-producing Klebsiella pneumoniae outbreak in a neonatal care center, molecular typing showed identical strains in both infected neonates and incubator mattresses, even after cleaning. Over half of incubator mattresses were contaminated with pathogens. The outbreak was controlled only after mattresses were replaced and disinfection protocols improved, directly linking mattress contamination to transmission and outbreak.⁴ |
| Chavignon et al. (2021) | In a tertiary NICU, all incubators remained contaminated with pathogenic bacteria despite standard disinfection. And all mattresses (100%) remained contaminated after disinfection. Two preterm neonates developed late-onset sepsis with bacteria previously isolated from their incubators, supporting a direct association between mattress contamination and infection.⁵ |
| Elkady et al. (2022) | In a NICU, MDR Klebsiella pneumoniae and Candida spp. strains were found in both neonates and their surrounding mattresses/incubators, as well as on healthcare workers’ hands. Homologous strains in neonates and environmental surfaces confirmed transmission pathways involving mattresses and beds.¹³ |
| Jenkins & Sherburn (2008) and Sherburn & Jenkins (2005) | Used cot mattresses, especially those without waterproof covers, accumulate nutrients that support bacterial growth and aerial release, including Staphylococcus aureus. These findings explain how mattresses can function as reservoirs and vectors for infection in infants.¹⁴,¹⁵ |
| Bokulich et al. (2013) and Hewitt et al. (2013) | NICU surfaces, including mattresses, harbor diverse and potentially pathogenic bacteria, with cleaning only partially reducing the microbial load. Highlight the ongoing risk of environmental transmission in neonatal units.¹⁶ ,¹⁷ |
| Guzman-Cottrill & Bryant (2025) | Provide evidence that mattresses and incubators are important sources of healthcare- associated infections in neonates; reinforcing the need for rigorous cleaning and monitoring.¹⁸ |
| Butin et al. (2019) | Sixty-two percent of incubators remained colonized with methicillin-resistant clone Staphylococcus capitis NRCS-A, a common cause of sepsis in NICUs, after disinfection. Mattresses and scales were most frequently colonized. Authors suggest reduced disinfection effectiveness was due to mattress seams, scale recesses, and non-immersible components, which allow biofilm formation and/or seal colonization. This, along with hand contamination, is likely to contribute to persistence of NRCS-A and transmission of S. capitis.¹⁹ |
In summary, studies use outbreak investigations, molecular typing, and mechanistic experiments to illustrate that mattress contamination in neonatal settings is a significant risk factor for infection and outbreaks, especially with multidrug-resistant organisms (MDROs). Improved cleaning, mattress replacement, and environmental monitoring are typical interventions. However, even with improved processes, complete microbial eradication does not occur and contamination persists. Incubator MIFUs are challenging to follow and require multiple steps with use of harsh disinfectants. One study confirmed that even following a two-step disinfection process for incubators, microbial contamination cannot be fully eliminated, particularly from mattresses.²¹ This highlights the inherent limitations and challenges of mattress disinfection with current MIFUs.
Practical And Effective Intervention: Mattress Barriers
There are numerous obstacles with routine cleaning and disinfection of mattresses. Substantial evidence confirms microbial contamination persists on mattresses even after cleaning and disinfection due to several issues. Firstly, mattress covers are soft, porous surfaces and there is not a true disinfectant capable of soft surface disinfection. The U.S. Environmental Protection Agency (EPA) does not have disinfectant claims for soft surfaces and only allows for sanitization claims. This is one reason surface microbial contamination persists on mattress. Additionally, as evidence has proven, many mattresses have cracks and microtears, creating a surface ripe for biofilm development. These damaged surfaces are incapable of being properly cleaned. Even more troublesome is the inability to fully inspect infant mattresses due to sealed seams. And finally, complicated MIFUs can be difficult to follow, leading to breaches in reprocessing and continued mattress contamination.
One of the most promising interventions is to use launderable mattress barriers to cover mattresses. These barriers undergo a validated laundering process that removes nearly all microorganisms, including spores. The laundering process is equivalent to high-level disinfection used for medical device reprocessing, which removes 99.9999% of all microorganisms. Having a validated clean mattress barrier is a needed intervention to reduce microorganism transmission and infection rates. Additionally, using a mattress barrier provides an alternative to lengthy and arduous MIFUs for mattress reprocessing, which further reduces disinfectant damage and extends mattress lifespan. Lastly, when a validated clean mattress barrier is used, compliance with regulatory bodies is ensured with a simplified, standardized cleaning process.

Clinical evidence supports using launderable mattress barriers as an effective infection prevention strategy across all care settings. Studies from acute and long-term care settings, showed the use of launderable mattress and bed deck covers resulted in an up to 50% reduction in hospital-onset Clostridioides difficile infections, even after adjusting for hand hygiene and length of stay.²²,²³ This demonstrates a clear link between launderable barriers and reduced infection rates.
Key Takeaway
Cracked, worn, or permeable mattress covers increase the likelihood of internal contamination, allowing organisms to persist and re-contaminate surfaces after cleaning. This cycle is well described in mattress contamination studies and reflects the inherent limitations of current mattress use and practices. Impermeable mattress covers are critical for preventing fluid and pathogen penetration, reducing the risk of mattress contamination and subsequent HAIs. Infections in the vulnerable neonatal population are devastating and without addressing the glaring mattress contamination problem, we continue to ignore a critical environmental reservoir. Impermeable, launderable mattress barriers should be established as standard of care, providing a validated and practical solution to this
long-standing gap in infection prevention.
For questions or comments, please contact Deva Rea MPH, BSN, RN, CIC
at Drea@trinityguardion.com
References
- Cura, C., Ozen, M., Kara, A. A., Alkan, G., & Cetin, E. S. (2016). Health care–associated infection
surveillance in a tertiary neonatal intensive care unit: A prospective clinical study after moving to a new
building. American Journal of Infection Control, 44(1), 80–84. https://doi.org/10.1016/j.ajic.2015.07.032 - Nishihara, Y., Zaniletti, I., Zenge, J., et al. (2025). Epidemiology of bacterial and fungal infections among
level IV neonatal units in North America. Journal of Perinatology. - An Assessment of Sepsis in the United States and its Burden on Hospital Care. Rockville, MD: Agency for
Healthcare Research and Quality; September 2024. AHRQ Pub No. 24-0087. - Cadot L, Bruguière H, Jumas-Bilak E, et al. Extended Spectrum Beta-Lactamase-Producing Klebsiella
Pneumoniae Outbreak Reveals Incubators as Pathogen Reservoir in Neonatal Care Center. European
Journal of Pediatrics. 2019;178(4):505-513. doi:10.1007/s00431-019-03323-w. - Chavignon M, Reboux M, Tasse J, et al. Persistent Microbial Contamination of Incubators Despite
Disinfection. Pediatric Research. 2021;90(6):1215-1220. doi:10.1038/s41390-021-01407-8. - FDA. Covers for Hospital Bed Mattresses: Learn How to Keep Them Safe. Updated 2017. Available at:
https://www.fda.gov/medical-devices/hospital-beds/covers-hospital-bed-mattresses-learn-how-keep-
them-safe - Sehulster LM, Chinn RYW, Arduino MJ, Carpenter J, Donlan R, Ashford D, Besser R, Fields B, McNeil MM,
Whitney C, Wong S, Juranek D, Cleveland J. Guidelines for environmental infection control in health-care
facilities. Recommendations from CDC and the Healthcare Infection Control Practices Advisory
Committee (HICPAC). Chicago IL; American Society for Healthcare Engineering/American Hospital
Association; 2004. - Creamer E, Humphreys H. The Contribution of Beds to Healthcare-Associated Infection: The
Importance of Adequate Decontamination. The Journal of Hospital Infection. 2008;69(1):8-23.
doi:10.1016/j.jhin.2008.01.014. - Viana Rel H, dos Santos SG, Oliveira AC. Recovery of Resistant Bacteria From Mattresses of Patients
Under Contact Precautions. American Journal of Infection Control. 2016;44(4):465-9.
doi:10.1016/j.ajic.2015.10.027. - Bousquet A, van der Mee-Marquet N, Dubost C, et al. Outbreak of CTX-M-15-producing Enterobacter
Cloacae Associated With Therapeutic Beds and Syphons in an Intensive Care Unit. American Journal of
Infection Control. 2017;45(10):1160-1164. doi:10.1016/j.ajic.2017.04.010. - Weber DJ, Rutala WA, Miller MB, Huslage K, Sickbert-Bennett E. Role of Hospital Surfaces in the
Transmission of Emerging Health Care-Associated Pathogens: Norovirus, Clostridium Difficile, and
Acinetobacter Species. American Journal of Infection Control. 2010;38(5 Suppl 1):S25-33.
doi:10.1016/j.ajic.2010.04.196. - Meda M, Virgincar N, Gentry V, et al. Clostridium difficile infection in pregnant and postpartum women in
2 hospitals and a review of literature. Am J Infect Control. 2019;47(1):e7-e14.
doi:10.1016/j.ajic.2018.06.001 - Elkady MA, Bakr WMK, Ghazal H, Omran EA. Role of Environmental Surfaces and Hands of Healthcare
Workers in Perpetuating Multi-Drug-Resistant Pathogens in a Neonatal Intensive Care Unit. European
Journal of Pediatrics. 2022;181(2):619-628. doi:10.1007/s00431-021-04241-6. - Jenkins RO, Sherburn RE. Used Cot Mattresses as Potential Reservoirs of Bacterial Infection: Nutrient
Availability Within Polyurethane Foam. Journal of Applied Microbiology. 2008;104(2):526-33.
doi:10.1111/j.1365-2672.2007.03609.x. - Sherburn RE, Jenkins RO. Aerial Release of Bacteria From Cot Mattress Materials and the Sudden Infant
Death Syndrome. Journal of Applied Microbiology. 2005;98(2):293-8. doi:10.1111/j.1365-
2672.2004.02456.x. - Bokulich NA, Mills DA, Underwood MA. Surface Microbes in the Neonatal Intensive Care Unit: Changes
With Routine Cleaning and Over Time. Journal of Clinical Microbiology. 2013;51(8):2617-24.
doi:10.1128/JCM.00898-13. - Hewitt KM, Mannino FL, Gonzalez A, et al. Bacterial Diversity in Two Neonatal Intensive Care Units
(NICUs). PloS One. 2013;8(1):e54703. doi:10.1371/journal.pone.0054703. - Guzman-Cottrill JA, Bryant KA. Keeping Your Neonatal Intensive Care Unit Clean: The Hospital
Environment as a Potential Source of Health Care-Associated Infections. Clinics in Perinatology.
2025;52(1):1-14. doi:10.1016/j.clp.2024.10.001. - Butin, M., Dumont, Y., Monteix, A. et al. Sources and reservoirs of Staphylococcus capitis NRCS-A inside
a NICU. Antimicrob Resist Infect Control 8, 157 (2019). https://doi.org/10.1186/s13756-019-0616-1 - Yu, M., Cross, K., Petrich, A., & Fish, J. (2016). Crib mattress investigation: Assessing cover permeability
and bacterial growth. American Journal of Infection Control, 44(7), 837– - https://doi.org/10.1016/j.ajic.2015.12.014
- Watkin S, Dunn H, Ready D, et al. Two-step or one-step – are all methods for neonatal incubator
decontamination equal?. J Hosp Infect. 2024;153:50-54. doi:10.1016/j.jhin.2024.07.012 - Hooker, Edmond A. et al. Decreasing Clostridium difficile health care–associated infections through use
of a launderable mattress cover American Journal of Infection Control, Volume 43, Issue 12, 1326 –
1330h. https://pmc.ncbi.nlm.nih.gov/articles/PMC4679628/ - Hooker EA, Mallow PJ, McKinney C, Gnoni ML, Fernandez Gonzales F. Use of a Launderable Bed Barrier
and Antibiotic Stewardship to Decrease Hospital Onset Clostridioides difficile Infections in an Acute
Care Hospital: A Retrospective Pre/Post Case Study. JHEOR. 2019;6(3):196-202.